
Świadomość aspektów zdrowia jako warunek rozwoju regionów zdrowia
Summary
Health is the most desirable value in modern society and the crucial aspect of a region as a place to live and rest. The concept of a health region is seen as a tool to increase the attractiveness of a place. The Pomeranian region is considered to have the potential to develop itself as a health region. It should be analysed, if the awareness of health issues is already present within the region. The empirical research shows that most themes discussed in the literature as preconditions for developing a health region are existing, while simultaneously several obstacles to achieve this goal still exist.
Bialk-Wolf Anna, Pechlaner Harald, Nordhorn Christian, Zacher Daniel
Awareness of health issues in the Pomeranian region as precondition for developing the health region
Introduction
The concept of a health region is mostly recognised as a tool to increase the attractiveness of a place for both residents and tourists [Volgger et al. 2015]. However, the existence of evidence how to develop and promote such a region is still sparse. The aim of this paper is an attempt to answer the question, if the awareness of health issues in the Pomeranian region is present and if we can regard this as a precondition for developing the health region.
This paper is organised as follows: After a short presentation of the theoretical background concerning the subjects of health and health region, the Pomeranian region is presented. GABEK®, which is the methodological tool applied in this study, is introduced and described. Finally, the findings from the empirical research are provided.
Theoretical Framework
During the last decades, health has become one of the most desirable values in modern society and culture. The pursuit, restoring, maintaining, and enhancing of health are key issues in the public debate [Crawford 1993]. Health aspects of various features of contemporary life are often debated and are the favourite subject of our small-talks with friends, especially when we are getting older. [Bjӧrklund, Svensson, Read 2006: 141]
Health means ‘feeling fine’, where we focus on experiences of positively valued feelings or as ‘ability to act’, where the meaning of health is expressed in terms of a person’s ability to act in a desirable way (from the person’s own point of view) or to live a life according to one’s own preferences. This theme has three slightly differing sub-themes: Being able to choose for oneself, being able to exercise control over one’s life and being able to actively partake in activities’’. Health can also be seen as an objective state of body and/or mind, suggesting objective matter-of-fact health criteria or as lack of disease, whereas disease is defined by the Oxford Dictionary as ‘disorder of structure or function in an organism that produces specific symptoms and is not the result of physical injury’ [as cited in Brüssow 2013: 342].
If we think about health, we can consider it as a continuum, where around a value of 0 is an indifference zone, where the person feels neither particularly healthy nor definitively ill. It is interesting, that numerous scoring systems exist to describe grades for many diseases, but little scoring systems for assessing health levels [Brüssow 2013: 344].
Even though there is no common definition of health, we should consider the definition set out in 1948 by the World Health Organisation: „Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”. This paradigm was groundbreaking, because it encompassed physical as well as mental and social aspects of health. One should also not overlook the fact, that during this time the health situation was completely different, because morbidity mainly featured infectious diseases. Contrarily, today chronic diseases are the main reason for mortality and they are much more prevalent.
Over time the debate on human health concepts has been dominated by two opposing views, which have been tagged biomedical/biostatistical/naturalism and normativism/holistic. Central to both approaches is the question of: how entities made up of several parts (systems) should be investigated: separately for every part or together, whether values influence our notion of health [Bjӧrklund, Svensson, Read 2006: 142-143].
The first view is biomedical and it is a reductionist view. This theory of health was built around the core concepts of ‘biological functioning’ and ‘statistical normality’. Health is seen as a normal functioning of the various parts of an organism. An organ or an organ system is healthy when it functions in accordance with a statistically determinable species design. According to this theory, disease is a type of internal state that reduces one or more functional abilities below this species-typical ability. When disease is absent, health is by definition present. The criteria, which determine, if health is absent or present are matter-of-fact and objective. This method is a positivistic view of science, which emphasizes what can be objectively measured and observed. Reality and specifically health are therefore a well-defined and objective state that is not influenced by the observer. Naturalists consider health a ‘natural’ and objective state, that is not subject to human values [Bjӧrklund, Svensson, Read 2006: 142; Svensson, Hallberg 2011].
They claim that natural sciences are sufficient to analyse health in its entirety. This approach is a descriptive one: health is viewed as an objective category ‘out there’ that can be described by various measurements. Health is normally assessed by experts, which use knowledge from natural sciences. Health is considered an abstract object that can be evaluated for all people by making use of the same procedures and methods. One of the most important concepts of health was stated by Boorse [1977], who stated in his definition of health explicitly that it is a ‘value-free theoretical notion’. [as cited in Bjӧrklund, Svensson, Read 2006: 142].
The opposing view, which is often spoken of as holistic, is socially oriented. It had a large impact on health discussions and health discourses during the recent decades. In this view health pertains to a person as a whole, rather than to some part of her/his body. The analysis of health should be placed within a social, not a biological, context. In Nordenfelt’s theory, which has been especially influential on Swedish occupational therapy, health refers to a person’s ability to reach her/his vital goals – that is, the goals that the person needs to reach to be happy. As a result, the determination of deciding the health-status is not given by objective facts. It also means that health is not the same as the absence of disease. Holists always consider the complete system, not only single parts. Also the links and interactions of the parts of a system and between different systems are important aspects for holism. A holistic way to look at health means that peoples’ experiences, thoughts, feelings, emotions, as well as other phenomena that cannot be measured, are included in the concept of health. Body and soul are not considered as separate entities, but as closely connected and health is regarded as a complex system that can always be improved. Humans are only considered as completely healthy, if they have managed to achieve all of their vital aims. Such an expanded view of health seems to be necessary in order to understand the pattern of diseases in modern society. It is obvious that the increasing wealth in society contributes to the development of new types of chronic diseases, so called diseases of wealth. Social and behavioural sciences relate these diseases to peoples’ ways of living and their choices of lifestyle. These diseases are therefore called lifestyle diseases [Bjӧrklund, Svensson, Read 2006: 142-143; Svensson, Hallberg 2011].
Since the WHO definition of health from 1948, the need for a dynamic description of health that highlights the human capacity for individual resilience and for coping with new situations was more and more required. In 2011 a new concept of health was introduced and health was defined “as the ability to adapt and to self manage, in the face of social, physical and emotional challenges’ [as citied in Huber et. al 2016: 1].
This new approach was proposed because the traditional one from the WHO was considered as no longer adequate. This new concept was developed at an international conference for experts held in the Netherlands in 2009. To support this concept of health, an interesting study was conducted by Huber et. al 2016.
The aim was to elaborate perceived indicators of health in order to make the concept measurable. The study considered three research questions:
- What do the various stakeholders consider to be positive and negative elements of the new general concept of health, and which elements should be specified in more detail?
- What do different stakeholders consider to be indicators of health?
- Do these indicators represent the new concept of health?
Participants were stakeholders from seven main domains within healthcare: healthcare providers (physicians, nurses, physiotherapists), patients with a chronic condition, policymakers, insurers, public health professionals, citizens (as a representative reflection of society) and researchers from different professional backgrounds. The qualitative study involved 140 stakeholders; the survey 1938 participants.
The result of the qualitative study was the identification of 556 health indicators, categorised into six dimensions: bodily functions, mental functions and perception, spiritual/existential dimension, quality of life, social and societal participation, and daily functioning [Huber et. al 2016: 7]. The quantitative study showed all stakeholder groups considering bodily functions to represent health, whereas for other dimensions there were significant differences between the groups. Moreover, patients considered all six dimensions almost equally important, thus preferring a broad concept of health. In order to prevent confusion with health as ‘absence of disease’, the authors propose the use of the term ‘positive health’ for the broad perception of health with six dimensions.
This broad concept of health incorporates the basis for further considerations in this paper. As health is the desirable value, it can be seen as a factor that influences decisions about the place of residence. Regions with a high quality of health service and an intact environment are also more appealing for tourists. The development of so-called “health regions” is a focus of interest for many European governments. It can also be seen as a tool to attract international patients with regard to medical tourism[1] [Connell 2006] and as an answer to some of the challenges that arise due to the liberal and global demand in health care [Volgger et al. 2015]. Pforr et al. [2011] suggest, that important factors in health region development comprise research, education, health prevention within companies, medical technology, hospitals, specialized primary health care providers, and health tourism. Volgger et al. discuss a health region as an instrument suitable both for health management and destination management, which can guarantee both public and private health, as well as aims related to tourism. The criteria for the establishment of health regions include common values, competencies, offers and common target groups in the area of health services to generate synergies, especially in promoting health tourism.
Table 1: Characteristics of idealized and fully developed health regions.
| Idealized and fully developed health region | |
| 1. Involvement of stakeholders | Broad organizational involvement of different stakeholder groups |
| 2. Benefits for local population | Goal is to ensure high quality health care for all local residents and tourists |
| 3. Visualization of the health region | Visualization as health region that serves both residents’ and tourists’ purposes |
| 4. Organization program present? | Specific organization with program |
| 5. Executing personnel | Specific personnel |
| 6. Communication channels present
| Specific internal and external communication channels |
Source: Volgger et al. 2015: 328
As one of the elements needed for developing a health region is a common culture (Volgger et al. 2015) and because furthermore culture can be defined as a “value system, which is shared by members of a local or regional area” [Cook et al. 1997: 488], the attitude to health issues can be regarded as precondition for developing a health region. This poses the central question of this paper: “What is the awareness of health issues and how can it contribute to the development of a health region?” The second aim of this study is an attempt to provide an answer to the question, what the understanding of the health region between important stakeholders in Pomerania is.
The literature overview shows that a large number of different aspects has to be considered when analyzing health and health region. The authors propose a conceptual framework [in figure 1] to provide a basis for the empirical research. Awareness of health is one of the common values in the region, which shapes the development of the health region and in turn is later influenced by the established health region. Nevertheless the development of a health region is a continuous process. Therefore health region can be seen as a dynamic concept that is influenced by and directly influences the mentioned criteria such as competences, offers and target groups.

Figure 1: Theoretical framework
Source: own elaboration based on Volgger et al. 2015, Huber et. al 2016.
Pomeranian Region
The Pomeranian region is situated in the northern part of Poland, on the southern coast of the Baltic Sea. One of the main assets of the region is its favourable geographical situation, which provides excellent transport links.
The region covers a total area of 18,310 square kilometres and it is home to a population of 2.31 mln (2015). The Pomeranian urban area, which comprises its biggest cities Gdansk, Slupsk, Sopot, Gdynia, accounts for 64.4 percent of the region’s population. There are 1512 tourist accommodation establishments. The population density amounts to 12,693,400 students attending 27 higher education institutions.
Regarding the potential to consider this region as a health region, it is also important that the life expectancy amounts to 74.2 years for males and 81.4 years for females. There are 55 general hospitals and 21.4 doctors for every 10,000 residents [Pomorskie Voivodship in Figures 2016], which is approximately the average level of Poland.
As regional recipe for success the following factors can be mentioned: seaside location on the crossroads of main European transport corridors; consistent investments in infrastructure, science and business; young, ambitious and excellently educated staff; exceptionally attractive place to live.
These aspects contribute directly to the touristic attractiveness of the region. Meanwhile, tourism intensity in the region is seasonal. In 2015 2439 thousand inbound tourists and 452 thousand international ones visited this region – the latter mainly from Germany, Norway, Sweden, Great Britain and Russia.
Methodology
In order to deal with the question of the awareness of health issues as precondition for developing the health region, eight interviews have been conducted in April and Mai 2016.
The interviews were analyzed using the GABEK® method (GAnzheitliche BEwältigung sprachlich erfasster Komplexität, or holistic management of complex material transmitted verbally): “While still relatively unknown […], GABEK has already been used in several business and social science studies” [Pechlaner, Volgger 2012]. The method is based on Gordon Pask’s conversation theory and Carl Stumpf’s theories of a phenomenological nature [Raich 2008; Stumpf 1939]. “This phenomenological orientation of GABEK® requires the collection of perceptions through open qualitative interviews; then, on these raw data a keyboard-based analysis is performed. By transforming statements into networks of interrelated keywords, GABEK® allows the extraction of the main messages, as well as the capture of a phenomenon’s evaluation and its perceived causes and effects” [Pechlaner, Volgger 2012]. According to Zelger, the inventor of the GABEK® method, “the personal viewpoints of the interviewee are linked by means of GABEK®, they are placed on top of each other and organized. Notes, quotations, texts, or even entire fields of knowledge are thus placed in a transparent compact map of ideas, thereby linking opinions, experience, knowledge, values, and emotional attitudes to one another in ‘term graphs,’ […] ‘impact nets,’ etc. […] The deeper structure becomes transparent so that connections can be understood, options evaluated, goals created, and trend developments recognized early on” [Zelger 2002: 6].
In that manner, GABEK® combines a qualitative approach with a traceable and clear analytic process [Pechlaner, Volgger 2012]. The suitability of GABEK® was already proven in several studies in social sciences [Raich 2008; Pechlaner, Volgger 2012; Pechlaner et al. 2016]. GABEK® is one hand based on clear rules, which minimize the subjective influence, on the other hand it offers researches freedom to implement new fields of research. In the end, “GABEK® produces an elegant visual representation of raw data and thus facilitates its interpretation” [Pechlaner, Volgger 2012: 930].
For this study, Network Graphics were created with the software tool WinRelan, which is based on the GABEK® method. Through the process of coding, transcripts are represented in the form of keywords. In this manner, sentences are represented as a set of terms and whole texts as a large, complex conceptual network. In this way, the main ideas and aspects of the interviews can be illustrated. In addition, terms of the interviews can be reduced to these, which show at least a connection for several times – this leads to a significant and clear presentation – and will always be mentioned in the upcoming network graphics.
Empirical Research
The eight interview partners had been selected based on their crucial role in different fields pivotal for the aim of this study. These sectors are: self-government responsible for tourism and health (interviews 3, 4, and 5), owners of clinics who are simultaneously active in health associations and foundations (2, 6, and 7), public health institution (1), research institute (8). The approximately half-hour long interviews have been conducted in Polish and have been audio taped and transcribed. The interview questionnaires have been semi-structured and have covered the following issues: meaning of health, health in the regional context, stakeholders of health in the region, role of inhabitants in creating the health region.
The empirical research has shown the connotation with the term “health”. Figure 2 presents a net graph, which displays the perceived important issues around the subject “health”.

Figure 2: Network Graphic „Health”
Source: own illustration, created with GABEK®.
Firstly, one must underline, that education seems to be a very important factor influencing the health habitants in the region. “School is the most important factor. School forms us. Education – already starting in kindergarten – plays a crucial role in our later habits referring to hygiene, diet, and sport activities. Moreover, if we are well educated, we are also able to take part in health promotion activity. That is why the basis is built by education” (5). As we can also depict from figure 2, the education of inhabitants is crucial for health and it should be encouraged through self-government.
Typical for many interviewees from companies and research institutions was, that they leave the task of promotion of health to self-government and see this institution as a crucial player in increasing the awareness of health in society.
Social and mental health are also mentioned (1, 3, and 4). “If we concentrate only on physical aspects of health, we are doomed to fail” (4), underlines one person from self-government. “If we feel good, we are healthy” (3), adds another interviewee, which also supports the broad concept of health. The next statement indicates another issue: “Physical activity is also connected with health. We can say that health equals sport. Healthy food and diet add up to health. Health is activity” (5). Health is also an aspect of beauty, hygiene and culture (6) and luck (7).
In summary it can be stated, that many different aspects of health are recognised, which stay in line with the broad definition of health described at the beginning of this paper.
Next we take a closer look at the term “health region”, which is presented in the next network graphic (Figure 3).
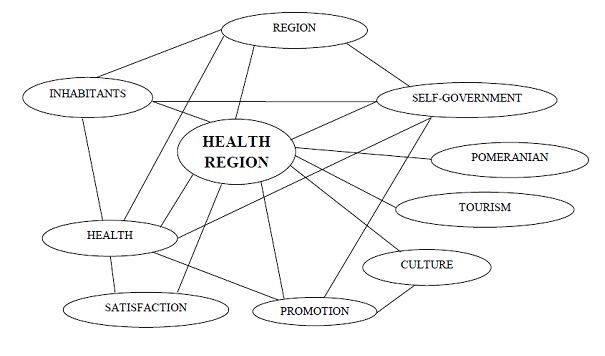
Figure 3: Network Graphic „health region”
Source: own illustration, created with GABEK®.
The goal of developing the health region is the improved satisfaction of inhabitants and their quality of life. Health region means that there “live healthy people, as well as well educated people, with outstanding hospitality, good health care availability and ecological engagement. In addition, unpolluted air and water, clean forests and good public traffic play also an important role. Awareness of the society – infrastructure – a place, where we can live healthily and rest” (5).
Culture as another pivotal issue has been mentioned (6). Interesting cultural offers should attract tourists and can be used for the promotion of the region. The task of promotion belongs to the self-government. One of the interviewees (4) underlined aspects of the health region and specified these as: healthy environment, safety regarding good hospitals and health services, self-government is “health” oriented. Safety seems also to be one of the important connotations with the health region. ”A feeling of safety can be seen as condition for spending money” (6) – added one of the interviewees. Another interviewee supports this with the following statement: “A health region must provide safety with regard to health services, be a place where people are content and be a good place for healing” (3).
Interviewees also underlined, that the level of awareness of the society is crucial for the chance to develop the health region. If it is high enough, the need to protect and support health should be present in different areas such as: own health, environment, education or health services (8). Competitiveness between suppliers of health services can also lubricate the developing of the health region, because it forces progress and a higher quality of products (6).
The analysis of the interviews allows to summarize, that the following stakeholders belong to the health region: health service, high schools, education, association and foundation, patient organisation, inhabitants, health care. However, the cooperation between all stakeholders is crucial (3). This corresponds to many researchers, who underline that one of the obstacles for tourism development in Poland is a lack of cooperation.
Many medical students and medical high schools are inherent elements of the health region (3). This is not only because of the need for professionals, but also because universities and research are considered sources of innovation and create a vital environment for the creative development of health competences.
The satisfaction of inhabitants refers to the accessibility of health services, of being healthy and to the contentment with the quality of the health services. They should be characterised by a healthy life style. The observation that most people in the region are happy and rather content with the place of residence is optimistic (3).
Conclusion
In summary it can be stated, that the most important elements of health and stakeholders required for developing the health region are present in the Pomeranian region. “Awareness” was often mentioned in connotation with health and can be considered as precondition for developing the health region.
Combining the theoretical consideration with the findings from the empirical research, we can say, that a successful health region is a geographically limited area with unpolluted natural environment, good medical and tourism infrastructure, an interesting cultural offer, well educated and healthy residents, who share common values and competencies and are aware of a broad set of health issues including bodily and mental functions, spiritual dimension, quality of life, social participation and daily functioning. To assure and further develop these assets, there has to be an active and ongoing commitment to the topic of health among various stakeholders. This should be expressed in a cooperation between broad ranges of stakeholders, especially from fields such as: education, research, medical technology, health prevention, health care providers, local population (who benefit from the existence of the health region), policy and health tourism. The region has the reputation of “being safe” and offers its services both to the local population and the selected target group of tourists. It has visualization, marketing and communication channels, as well as a specific organizational structure with program and staff.
Many of the aspects mentioned can also be seen as political goals of local, regional or national governments. This intends that the proclamation of a (institutional) health region in a geographically defined area can also help to develop the mentioned aspects of a successful health region. There might be a need of public funding for the concept of health region as long as its goals go along with public interest.
These overall results are now reflected in the Pomeranian region. The study has highlighted several problems in the region. The Pomeranian region is perceived as a region with high potential, but a coordination of the efforts is urgently needed (4). We can also observe a lack of feeling to be one society (6). This is directly related to problems with cooperation and trust.
A lack of sufficient prevention is another important aspect (2). The need for prevention as an element of the health region is depicted, but there is still not enough engagement to implement this. In addition, a lack of information is seen as a challenge, especially in cases of illness (3). This causes a feeling of uncertainty which in turn increases the need for safety. This problem is connected with a deficit of doctors’ soft skills, who are often more interested in learning hard skills than acquire empathy. (3). One of the interviewees pointed to another problem with the following statement: “A lack of standards in health care and also plain ‘disorder’ are also problems of the health system we have here” (7).
Missing responsibility for one own’s health is seen as an obstacle for developing better health care. This is the area of politicians, who do not provide incentives for more self-care (7). The integration of society is one of the challenges that Pomerania is currently facing.
Further research could deal with a proposal for the region to better exploit the huge potential for developing the health region. Another interesting question could be the development of strategies to outline the task for different stakeholders to overcome the existing problems in the region.
Sposób cytowania: Bialk-Wolf Anna, Pechlaner Harald, Nordhorn Christian, Zacher Daniel, Awareness of Health Issues in the Pomeranian Region as Precondition for Developing the Health Region, [w:] Looking for Health, Fitness, and Beauty, Lubowiecki-Vikuk Adrian (red.), Studia Periegetica nr 2(16)/2016, s. 45-58.
Bibliography
Białk-Wolf A., 2010, Potencjał rozwojowy turystyki medycznej. Zeszyty Naukowe Uniwersytetu Szczecińskiego, Ekonomiczne Problemy Usług, 591(53): 653-662.
Bjӧrklund A., Svensson T., Read S., 2006, Holistic and biomedical concepts of health: A study of health notions among Swedish occupational therapists and a suggestion for developing an instrument for comparative studies, Scandinavian Journal of Occupational Therapy, 13: 141-150.
Brüssow H., 2013, What is health? Microbial Biotechnology, 6(4): 341–348.
Connell J., 2006, Medical tourism: sea, sun, sand and … surgery, Tourism Management, 27:1093-1100.
Cooke P., Uranga M.G., Etxebarria G., 1997, Regional innovation systems: Institutional and organisational Dimensions, Research Policy, 26: 475-491.
Crawford R., 1993, A cultural account of ‘health’: control, release, and the social body, Health and Wellbeing, 133-143.
Huber M., van Vliet M., Giezenberg M., Winkens B., Heerkens Y., Dagnelie P.C., Knottnerus J.A., 2016, Towards a ‘patient-centred’ operationalisation of the new dynamic concept of health: a mixed methods study. BMJ Open 2016;5:e010091.doi:10.1136/bmjopen-2015-010091.
Pechlaner H., Nordhorn C., Poppe X., 2016, Being a Guest: Perspectives of an Extended Hospitality Approach, International Journal of Culture, Tourism, and Hospitality Research. Special Issue. Will be published soon.
Pechlaner H., Volgger M., 2012, How to Promote Cooperation in the Hospitality Industry, International Journal of Contemporary Hospitality Management, 24 (6): 925 – 945.
Pforr C., Pechlaner H., Locher C., Jochrnann J., 2011, Region as Tourism Destination. A New Approach to Regional Development, Paper presented at the International Conference on Tourism. ICOT 2011, April 2011, Rhodes Island, Greece.
Pomorskie Voivodship in Figures 2016, Statistical Office
Raich M., 2008, Basic Values and Objectives regarding Money: Implications for the Management of Customer Relationships, International Journal of Bank Marketing, 26 (1): 25-41.
Stumpf C., 1939, Erkenntnislehre: Band 1., Leipzig: Johann Ambrosius Barth.
Svensson O., Hallberg L.,Hunting for health, well-being, and quality of life International Journal of Qualitative Study Health Well-being, 6: 7137 – DOI: 10.3402/qhw.v6i2.7137.
Volgger M., Mainil T., Pechlaner H., Mitas O., 2015, Health region development from the perspective of system theory. An empirical cross-regional case study, Social Science & Medicine, 124: 321-330.
Zelger J., 2002, Gabek – Bd. I: Von der Problemstellung zum Zwischenbericht [GABEK – Volume 1: From the Problem to the Preliminary Report]. Innsbruck: Innsbrucker Universitätsverlag.
[1] “Medical tourism is travelling abroad with the intent to make use of medical treatment for the purpose of preserving life, enhancing the quality of life or improving one’s appearance; because of lower cost, better quality or the inaccessibility of some procedure at the place of residence (resulting from a lack of personnel, knowledge technical equipment and procedures, or long waiting times or legal limitations) often combined with sightseeing the visited place.” [Białk-Wolf 2010: 655]

